- Case Report
- Open access
- Published:
Two cases of spontaneous hyphema after posterior chamber phakic intraocular lens implantation
BMC Ophthalmology volume 25, Article number: 91 (2025)
Abstract
The implantable collamer lens (ICL, STAAR Surgical Co.) surgery is popular for its effectiveness and safety, but it carries potential risks. This study presents two unreported cases of hyphema after ICL surgery, highlighting the need for prompt investigation and management of both hyphema and IOP to prevent ocular damage.
Introduction
The V4c EVO Visian Implantable Collamer Lens (ICL) (Staar Surgical AG, Nidau, Switzerland) is a posterior chamber phakic lens with a 360 μm central port, eliminating the need for iridotomy and reducing risks such as elevated intraocular pressure (IOP) [1, 2]. Based on this design, ICL surgery has gained significant popularity worldwide. Although ICL surgery is not classified as a laser refractive procedure, it offers a crucial alternative for patients who are not candidates for laser treatments, such as those with thin corneas or high refractive errors [3,4,5,6,7,8]. It has been observed that despite its effectiveness in correcting moderate to high myopia [3,4,5,6,7,8], complications persist. This report presents two cases of hyphema following ICL-V4c surgery, which provide clinicians with valuable insights into ICL surgery and contribute to a more comprehensive understanding of how to optimise patient care and outcomes.
Case Presentation
Case 1
Chief Complaint: A 27-year-old visited the hospital for re-examination following ICL surgery.
Clinical Signs and Symptoms: She reported experiencing transient vision loss in her right eye lasting for one hour, without any identifiable trigger, five months post-surgery.
Medical History: She denied any history of trauma and had no significant past medical issues.
Examination: A physical examination revealed the following:
-
No facial injuries.
-
The conjunctiva of the right eye showed no signs of congestion, and the cornea appeared transparent.
-
Blood clots were visible in the anterior chamber and pupillary area.
-
A red membranous substance was found in the central hole of the V4c lens, along with a blood-like attachment on the posterior surface of the V4c lens.
-
The pupil was round, approximately 3 mm in diameter, with a positive (+) light reflex.
-
The lens was transparent.
Diagnostic findings included a noncontact tonometer (NCT) reading of 47.9 mmHg and anterior segment optical coherence tomography (OCT) showing an anterior chamber depth of 1.8 mm and a vault of 1.2 mm.
Preliminary Diagnosis: ICL surgery was performed in both eyes, right hyphema.
Treatment: Both eyes were immobilized. The patient was placed in the Semi-Fowler position. Topical instillation of 0.15% brimonidine eye drops, levofloxacin eye drops, and compound tropicamide eye drops were administered. Paracentesis of the anterior chamber and fluid drainage were performed multiple times. A physical examination conducted the next morning revealed the following:
-
Uncorrected distant visual acuity (UCDVA) in the right eye was 0.12.
-
No conjunctival congestion.
-
Mild corneal edema.
-
The ICLs were properly positioned.
-
Pigment on the ICL surface (+).
-
A small number of blood cells on the lens surface.
-
Blood clots in the middle and lower parts of the anterior chamber.
-
Enlarged pupils.
-
Weak light reflex (Fig. 1A).
Fig. 1 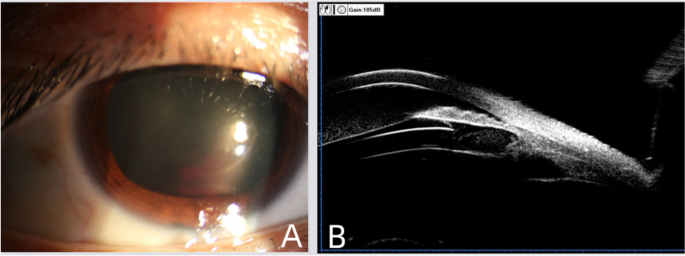
A Slit-lamp photography of the anterior segment taken on the first day after starting treatment administered in the emergency room. Pupillary dilation is due to the use of mydriatic drugs. B After 10 days of treatment, UBM showed that the ICL was well-positioned with a vault of 1.03 mm. The anterior chamber revealed punctate hyperechoic foci, suggesting blood cells floating in the anterior chamber, which can be clinically corroborated using the slit-lamp

Treatments, including anti-inflammatory therapy, intraocular pressure control, and immobilization, were continued.
Results: The patient was continuously observed and followed up. After 10 days, the patient was re-examined and reported no discomfort. Uncorrected visual acuity (UCVA) in the right eye was 1.0, the hyphema was absorbed, the ICL was in place, and the lens was transparent. Ultrasound biomicroscopy (UBM) suggested punctate hyper-echo in the anterior chamber (Fig. 1B).
Case 2
Chief Complaint: A 26-year-old female visited the hospital for a re-examination following ICL surgery.
Clinical Signs and Symptoms: She reported experiencing sudden blurred vision in the left eye for half an hour without any obvious cause, occurring 2 months post-ICL surgery in both eyes.
Medical History: She denied any history of trauma to the left eye and had no significant past medical history.
Physical examination:
-
Left eye visual acuity: hand motion (HM)/30 cm.
-
Oculus sinister (OS): 31 mmHg.
-
Dusty and pigmented keratic precipitate (KP) on the corneal endothelial surface (+++).
-
Central anterior chamber depth of approximately 3 corneal thicknesses (CT).
-
Peripheral anterior chamber depth of about 1/2 CT.
-
Tyndall effect (+++).
-
Cells (+++).
-
Inferior hyphema: approximately 2 mm.
-
Pupil diameter: approximately 3 mm, with a positive light reflex (+).
-
ICL in place, with surface opacity and pigmentation.
-
Hematocele in the central hole.
-
The vault and the fundus were not clear.
Preliminary diagnosis:
-
1.
Left hyphema.
-
2.
Secondary intraocular hypertension in the left eye.
-
3.
ICL surgery was performed in both eyes. Ultrasonography showed mild vitreous opacity in the left eye. The patient was hospitalized for observation. Both eyes were immobilized, and the patient was placed in the Semi-Fowler position. The following treatments were administered:
-
Intramuscular injection of spearhead pit viper hemocoagulase 1u.
-
Intravenous drip of 20% mannitol, 250 ml.
-
Topical instillation of 0.15% brimonidine eye drops and prednisone eye drops.
-
Treatment: Initially, the patient’s intraocular pressure was normal but later increased again, fluctuating between 35 and 38 mmHg, with recurrences of hyphema absorption after 2 days. During the observation period, fluid drainage of the anterior chamber was performed throughout the entire process. Topical instillation of brimonidine eye drops, brinzolamide, and timolol maleate eye drops was also administered to lower intraocular pressure. In addition, prednisone eye drops were given for anti-inflammatory therapy. Moreover, UBM showed moderate to strong homogeneous echo between the root of the iris at the 8–10 o’clock position and the intraocular lens (posterior chamber). After 2 days of observation, the patient’s visual acuity in the left eye recovered to 1.2, with intraocular pressure measuring 18.0 mmHg. The cornea was transparent, the central anterior chamber depth was measured, the Tyndall effect (+), and a small amount of bloody aqueous humor was observed below. The intraocular lens was clear and in place.
Result: After 7 days of topical instillation of eye drops for anti-inflammatory therapy and intraocular pressure reduction, blood cells were still visible in the anterior chamber, and intraocular pressure was maintained between 19 and 22 mmHg. Upon re-examination with UBM, a small amount of moderate to strong homogeneous echo was detected between the root of the iris at 8–10 o’clock and the intraocular lens in the posterior chamber (Fig. 2).

A Slit-lamp photography of the anterior segment taken 2 days after admission, showing blood in the anterior chamber. B Image of UBM examination taken after 1 week of treatment, revealing punctate hyperechoic foci in the anterior chamber suggesting blood cells floating
ICL-V4c implantation surgical procedure
In both cases, the same ophthalmic surgeon performed the ICL surgeries under topical anaesthesia with proparacaine hydrochloride eye drops. After sterilizing the ocular surface and applying a lid speculum, a 2.75 mm incision was made at the corneoscleral limbus. The ICL-V4c was inserted, and the viscoelastic agent was used to position it.
Discussion
Hyphema after ICL surgery has been rarely reported, despite ICL surgery being widely performed both domestically and internationally for many years. It is widely recognized in clinical practice for its safe and effective vision correction with fewer complications, making it the preferred surgical option recommended for correcting high myopia [4,5,6, 8, 9]. Currently, most cases of hyphema after ICL procedures reported in clinical practice are typically traumatic [10,11,12], a possibility ruled out by the two patients in this report who denied any history of trauma. The second patient experienced recurrent hyphema during the observation period, which was clearly unrelated to trauma. Non-traumatic hyphema is commonly associated with drug-related causes, local abnormalities such as inflammation, tumors, or hemangiomas, and systemic immune diseases like diabetes. Drug-related factorsmay involve oral administration of anticoagulant drugs, but neither of the patients reported in this study reported using systemic or topical medications that affect coagulation function. Local inflammation, including iris-ciliary inflammation, iris-ciliary hemangioma, or tumor, may be considered. However, neither patient in this case had a definitive diagnosis. The two patients did not have any immune inflammation, such as rheumatism, nor did they experience immune decline triggers, such as colds, before the onset of the disease. UBM did not reveal any obvious iris tumors or hemangiomas. Also, preoperative examinations did not show retinal hemangiomas or other predisposing factors that could lead to complicated iris hemangiomas. Uveitis-glaucoma-hyphema syndrome(UGH) [13, 14] is also considered a possible diagnosis with recurrent symptoms similar to those in Case 2. Its pathogenesis may be related to the intraocular lens not being smooth enough, causing prolonged friction with the iris and other tissues, leading to damage to the iris and other tissues. This condition is prone to recurrence, and in severe cases, the intraocular lens may need removal due to poor disease control. However, in pre-operative exams, no abnormalities were observed in this patient. The slit-lamp examination did not show signs typically associated with UGH, such as pigment dispersion, iris transillumination, or localized pigment deposition on the lens, which can result from friction between the intraocular lens and iris. Additionally, postoperative monitoring, including UBM, confirmed that ICL haptics were in the correct position. It is noticed that one paper by Zhang Weijie, Li Fang, Zhou Jibo reported [15] that UBM reveals the rupture of a ciliary body cyst, which is a potentially significant factor that may arise. However, in both of our cases, UBM examinations post-surgery did not show any obvious damage or rupture of the ciliary body. Besides, the fundus did not show macular edema. Moreover, neither of the two patients experienced recurrence after treatment, which does not entirely align with the diagnosis and predisposing factors of UGH.
Additionally, both patients in this case had long-term hyphema without any obvious precipitating factors following ICL surgery. Although the prognosis is good after treatment, high clinical attention should still be paid. Moreover, the ICL may still need to be removed if necessary to ensure the patients’ health. Therefore, the importance of regular re-examinations should be emphasized in clinical practice for patients who have undergone ICL surgery [16]. When hyphema symptoms appear, it is crucial to actively investigate the causes and promptly manage bleeding and intraocular pressure to prevent secondary damage to eye health from elevated intraocular pressure. In these cases, although the cause of bleeding is unknown, there is still a noticeable similarity between the two patients in that they are both females and experienced hyphema a long time after ICL surgery. Currently, there are no reported cases among male ICL patients, and there is insufficient evidence to determine whether it is related to factors such as the female menstrual cycle or arch height. Further observation is necessary to establish any potential correlations.
Given the rarity of hyphema after ICL surgery and the uncertainties regarding its cause in these cases, it is crucial for clinicians to take a careful approach in both preoperative planning and postoperative follow-up. Specifically, when selecting the appropriate ICL, clinicians should not only consider the anticipated vault height after surgery but also pay close attention to the UBM of patient results. It is important to evaluate the shape of the anterior segment, including the iris and ciliary body morphology, as well as factors such as haptic area, angle of haptic, and mechanical forces. By considering these additional factors, clinicians can make more informed decisions regarding ICL sizing, ultimately leading to a safer postoperative outcome for patients.
Data availability
The data that support the findings of this study are available from Chongqing Eye and Vision Care Hospital, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Chongqing Eye and Vision Care Hospital.
References
Amer AA, Ahmed Ghanem Abu El Wafa Ali E, Sayed Ahmed E, et al. Posterior-Chamber Phakic Implantable Collamer Lenses with and without a Central Hole: a comparative study. Clin Ophthalmol (Auckland). 2023;17:887–95. https://doiorg.publicaciones.saludcastillayleon.es/10.2147/OPTH.S405689.
Chen X, Miao H, Naidu RK, et al. Comparison of early changes in and factors affecting vault following posterior chamber phakic Implantable Collamer Lens implantation without and with a central hole (ICL V4 and ICL V4c). BMC Ophthalmol. 2016;16:161. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12886-016-0336-8.
Fern Ndez-Vega-Cueto L, Alfonso-Bartolozzi B, Lisa C, et al. Seven-year follow-up of posterior chamber phakic intraocular lens with central port design. Eye Vision. 2021;8:23. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s40662-021-00247-1.
Wan Q, He P, Wei R, et al. Long-term observation of V4c implantable collamer lenses implantation for moderate to extreme high myopia correction: five years follow-up. Eye (Lond). 2024;38:1933. https://doiorg.publicaciones.saludcastillayleon.es/10.1038/s41433-024-03046-9.
Amer I, Ziada HA, Elgazzar AF, et al. Safety and efficacy of implantable phakic contact lens versus implantable collamer lens in myopia correction. Med Hypothesis Discov Innov Ophthalmol. 2023;12(4):160–7. https://doiorg.publicaciones.saludcastillayleon.es/10.51329/mehdiophthal1482.
Albo C, Nasser T, Szynkarski DT, et al. A comprehensive retrospective analysis of EVO/EVO + implantable collamer lens: evaluating refractive outcomes in the largest single center study of ICL patients in the United States. Clin Ophthalmol. 2024;18:69–78. https://doiorg.publicaciones.saludcastillayleon.es/10.2147/OPTH.S440578.
Alabbasi OM, Vargas J, AL Mutlak M, et al. Spherical equivalent pre- and post-implantable collamer lens implantation in patients with myopia, hyperopia, and stable keratoconus. Saudi J Ophthalmol. 2023;37(4):327–30. https://doiorg.publicaciones.saludcastillayleon.es/10.4103/SJOPT.SJOPT_130_22.
陈越兮, 林丁, 张青松 et al. 有晶状体眼后房型人工晶状体植入术矫正中高度近视的远期临床观察[J]. 中华眼视光学与视觉科学杂志, 2020;22(3):7. https://doiorg.publicaciones.saludcastillayleon.es/10.3760/cma.j.cn115909-20190731-00210
Alfonso-Bartolozzi B, Fernandez-Vega-Cueto L, Lisa C, et al. Ten-year follow-up of posterior chamber phakic intraocular lens with central port design in patients with low and normal vault. J Cataract Refract Surg. 2024;50(5):441–7. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/j.jcrs.0000000000001379.
高阳. 任毅, 周奇志 %+ 重庆爱尔眼科医院 %+ 重庆爱尔眼科医院 重. 有晶状体眼后房型人工晶状体植入术后外伤性人工晶状体脱位一例[J]. 中华眼科杂志. 2018;54(9):700–2. https://doiorg.publicaciones.saludcastillayleon.es/10.3760/cma.j.issn.0412-4081.2018.09.014.
Winegar JW, Justin GA, Bower KS, et al. Traumatic aniridia after implantable phakic intraocular lens placement. J Cataract Refract Surg. 2018;44(9):1155–7. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.jcrs.2018.06.027.
Moshirfar M, Stagg BC. Traumatic dislocation of implanted collamer phakic lens: a case report and review of the literature. Open Ophthalmol J. 2014;8:24–6. https://doiorg.publicaciones.saludcastillayleon.es/10.2174/1874364101408010024.
Almasri KG, Pichi F. Uveitis-Glaucoma-Hyphema syndrome secondary to implantable collamer lens. Ocul Immunol Inflamm. 2024:1–4. https://doiorg.publicaciones.saludcastillayleon.es/10.1080/09273948.2024.2342386.
Dossantos J, Bade Y. Occult uveitis-Glaucoma-hyphema syndrome caused by PCIOL with Peripheral Capsular Tear. Case Rep Ophthalmol. 2024;15(1):383–7. https://doiorg.publicaciones.saludcastillayleon.es/10.1159/000538063.
Weijie Z, Fang L, Jibo Z. Anterior segment hemorrhage after implantable collamer lens surgery. Ophthalmology. 2024. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.ophtha.2024.06.015.
中华医学会眼科学分会眼视光学组. 中国有晶状体眼后房型人工晶状体植入术专家共识(2019年). 中华眼科杂志. 2019;55(9):652–7. https://doiorg.publicaciones.saludcastillayleon.es/10.3760/cma.j.issn.0412-4081.2019.09.005.
Acknowledgements
Appreciation is extended to each member of the team led by Professor Qizhi Zhou for their contributions to this case.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
Yang Gao (ORCID: 0000-0001-5536-3931): data collection, data analysis, and interpretation, manuscript writing, and revision according to the editorial suggestions of the office.Qizhi Zhou (ORCID: 0000-0001-7965-0257): research topic design, data analysis, interpretation, and participation in revising the discussion of the paper. Chenxue Liu (ORCID: 0000-0002-1585-4493): data analysis and interpretation, writing and approving the English manuscript version. Lili: data analysis, and interpretation.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Data are available from the corresponding author upon request.
Consent for publication
The content of this case report or any similar content has not been published elsewhere and is intended solely for publication in this journal. Written informed consent was obtained from the patients for the publication of this case report.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gao, Y., Liu, C., Li, L. et al. Two cases of spontaneous hyphema after posterior chamber phakic intraocular lens implantation. BMC Ophthalmol 25, 91 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12886-025-03904-4
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12886-025-03904-4